Archie was an adult dog with a known history of severe pulmonic stenosis. He was presented because of progressive exercise intolerance, weight loss, and intermittent episodes of heavy breathing. His owners also reported increased thirst and urination. On examination, he had a loud right basilar systolic murmur and mild abdominal fullness, but no obvious pleural effusion or severe respiratory compromise. Thoracic radiographs were performed to evaluate the severity of cardiac remodelling, pulmonary perfusion, and whether there was evidence of congestive heart failure or metastatic disease.
Three thoracic radiographs showed marked right-sided cardiomegaly. On the lateral views, there was increased sternal contact and dorsal displacement of the trachea. On the DV view, the cardiac silhouette had a classic reverse-D shape, consistent with marked right ventricular enlargement. The VHS measured 14.6. The caudal vena cava was subjectively enlarged and measured more than twice the height of the aorta, suggesting increased right-sided filling pressures. There was also mild leftward deviation of the mediastinum, likely reflecting main pulmonary artery bulging.
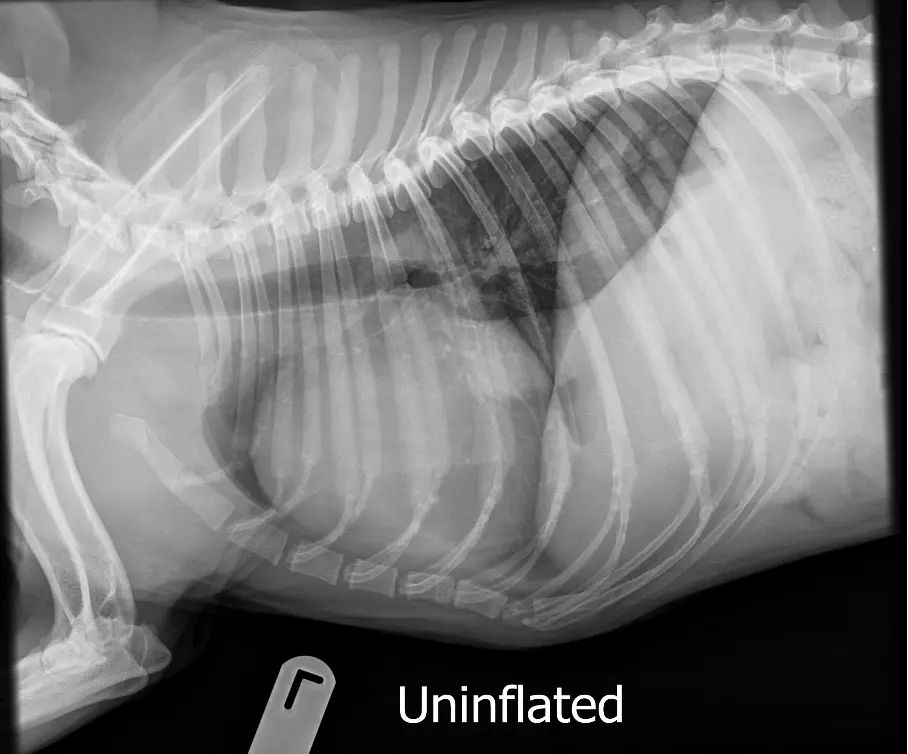
The pulmonary vessels were reduced in size throughout the visible lung fields, resulting in a generalised decrease in pulmonary opacity. This was compatible with reduced pulmonary blood flow secondary to severe right ventricular outflow obstruction. No pleural effusion, overt ascites, or pulmonary oedema was present. The thorax was otherwise unremarkable apart from incidental musculoskeletal changes.
The radiographic conclusion was that the marked right-sided cardiomegaly and small pulmonary vessels were compatible with the known severe pulmonic stenosis. The enlarged caudal vena cava suggested an early stage of right-sided congestive heart failure, even though there was not yet radiographic evidence of pleural effusion, hepatomegaly, or ascites.
Archie underwent repeat echocardiography, confirming severe valvular pulmonic stenosis with marked right ventricular hypertrophy and elevated transvalvular velocity. Because the anatomy was suitable, balloon pulmonary valvuloplasty was recommended. He was also started on supportive therapy for early right-sided congestion, including cautious diuretic therapy and exercise restriction while awaiting the procedure.
Balloon valvuloplasty was performed successfully, with a significant reduction in the pressure gradient across the pulmonic valve. Over the next month, Archie’s breathing improved, his stamina increased, and his abdominal fullness resolved. His resting respiratory rate remained normal at home, and his owners reported that he was more willing to exercise. Follow-up echocardiography showed persistent right ventricular remodelling, as expected, but improved right-sided loading conditions and no progression of congestive signs.
This case is a useful example of how severe pulmonic stenosis can be recognised radiographically. A reverse-D cardiac silhouette, marked right-sided cardiomegaly, small pulmonary vessels, and an enlarged caudal vena cava together strongly support severe right ventricular outflow obstruction with early right-sided heart failure.